






よむ、つかう、まなぶ。
資料5障害者権利条約の対日審査結果について (15 ページ)
出典
| 公開元URL | https://www.mhlw.go.jp/stf/shingi2/0000195428_00060.html |
| 出典情報 | 社会保障審議会 障害者部会(第133回 10/17)《厚生労働省》 |
ページ画像
ダウンロードした画像を利用する際は「出典情報」を明記してください。
低解像度画像をダウンロード
プレーンテキスト
資料テキストはコンピュータによる自動処理で生成されており、完全に資料と一致しない場合があります。
テキストをコピーしてご利用いただく際は資料と付け合わせてご確認ください。
CRPD/C/JPN/CO/1
(a)
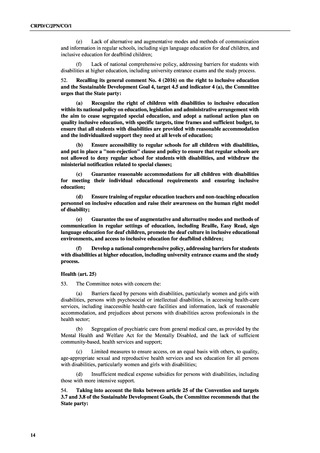
Ensure quality and gender-sensitive health-care services for all persons
with disabilities, including by ensuring the implementation of accessibility standards
and the provision of reasonable accommodation by public and private health providers;
(b)
Guarantee that information is provided in accessible formats for persons
with disabilities, including in Braille, sign language and Easy Read, regarding health
services;
(c)
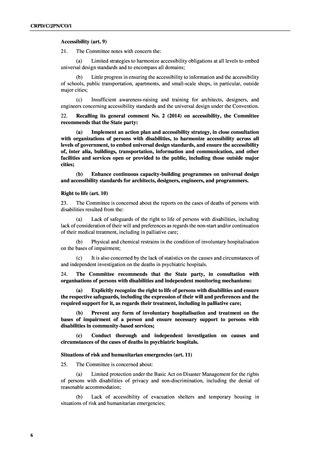
Integrate a human rights- model of disability into the training of health
professionals, emphasizing that all persons with disabilities have the right to free and
informed consent for any medical and surgical treatment;
(d)
Develop, in close consultation with organizations of persons with
psychosocial disabilities, non-coercive, community-based mental health support, and
adopt the necessary legislative and policy measures to dismantle systems that separate
mental health care from general medical care;
(e)
Ensure that high-quality, age-appropriate sexual and reproductive health
services and comprehensive sexuality education are inclusive of and accessible to all
persons with disabilities, in particular women and girls with disabilities;
(f)
Establish a mechanism of medical expense subsidies based on the person’s
capacity to cover the costs, and expand these subsidies for all persons with disabilities,
including those with more intensive support.
Habilitation and rehabilitation (art. 26)
55.
The Committee notes with concern:
(a)
The shortage of comprehensive and cross-sectoral habitation and rehabilitation
services, particularly to support children and outside of major cities;
(b)
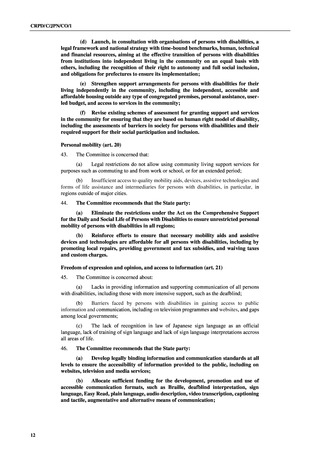
The emphasis of the medical model in habilitation and rehabilitation
programmes, and differences in support based on type of disability, sex and region.
56.
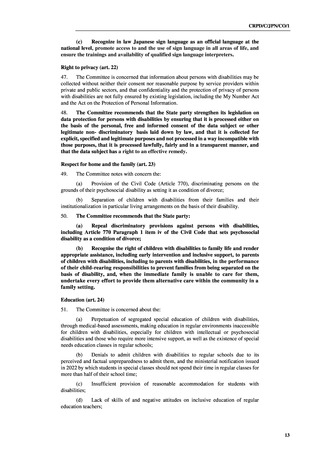
The Committee recommends that the State party:
(a)
Adopt measures to secure access to comprehensive and cross-sectoral
habilitation and rehabilitation services, programmes and technology, within their
community, and in all the State party;
(b)
Expand habilitation and rehabilitation systems, taking into account the
human rights model of disability, and ensure that all persons with disabilities have
access to these services based on their individual requirements.
Work and employment (art. 27)
57.
The Committee is concerned about:
(a)
The segregation of persons with disabilities, particularly persons with
intellectual or psychosocial disabilities, in sheltered workshops and employment-related
welfare services, with low wages and limited opportunities to transition to the open labour
market;
(b)
Barriers to employment faced by persons with disabilities, including
inaccessible workplaces, the insufficient support and individualized accommodation in both
the public and private sectors, limited mobility assistance and information provided to
employers about the capabilities of persons with disabilities;
(c)
Gaps in the local governments and the private sector concerning the
employment rate system for persons with disabilities, as provided by the Act for the
Promotion of Employment for Persons with Disabilities, and lack of a transparent and
effective monitoring mechanism to ensure its implementation;
(d)
Restrictions concerning the use of personal assistance services for persons who
require more intensive support at work.
15
(a)
Ensure quality and gender-sensitive health-care services for all persons
with disabilities, including by ensuring the implementation of accessibility standards
and the provision of reasonable accommodation by public and private health providers;
(b)
Guarantee that information is provided in accessible formats for persons
with disabilities, including in Braille, sign language and Easy Read, regarding health
services;
(c)
Integrate a human rights- model of disability into the training of health
professionals, emphasizing that all persons with disabilities have the right to free and
informed consent for any medical and surgical treatment;
(d)
Develop, in close consultation with organizations of persons with
psychosocial disabilities, non-coercive, community-based mental health support, and
adopt the necessary legislative and policy measures to dismantle systems that separate
mental health care from general medical care;
(e)
Ensure that high-quality, age-appropriate sexual and reproductive health
services and comprehensive sexuality education are inclusive of and accessible to all
persons with disabilities, in particular women and girls with disabilities;
(f)
Establish a mechanism of medical expense subsidies based on the person’s
capacity to cover the costs, and expand these subsidies for all persons with disabilities,
including those with more intensive support.
Habilitation and rehabilitation (art. 26)
55.
The Committee notes with concern:
(a)
The shortage of comprehensive and cross-sectoral habitation and rehabilitation
services, particularly to support children and outside of major cities;
(b)
The emphasis of the medical model in habilitation and rehabilitation
programmes, and differences in support based on type of disability, sex and region.
56.
The Committee recommends that the State party:
(a)
Adopt measures to secure access to comprehensive and cross-sectoral
habilitation and rehabilitation services, programmes and technology, within their
community, and in all the State party;
(b)
Expand habilitation and rehabilitation systems, taking into account the
human rights model of disability, and ensure that all persons with disabilities have
access to these services based on their individual requirements.
Work and employment (art. 27)
57.
The Committee is concerned about:
(a)
The segregation of persons with disabilities, particularly persons with
intellectual or psychosocial disabilities, in sheltered workshops and employment-related
welfare services, with low wages and limited opportunities to transition to the open labour
market;
(b)
Barriers to employment faced by persons with disabilities, including
inaccessible workplaces, the insufficient support and individualized accommodation in both
the public and private sectors, limited mobility assistance and information provided to
employers about the capabilities of persons with disabilities;
(c)
Gaps in the local governments and the private sector concerning the
employment rate system for persons with disabilities, as provided by the Act for the
Promotion of Employment for Persons with Disabilities, and lack of a transparent and
effective monitoring mechanism to ensure its implementation;
(d)
Restrictions concerning the use of personal assistance services for persons who
require more intensive support at work.
15