



















よむ、つかう、まなぶ。
資料1-2 調査結果報告書 (19 ページ)
出典
| 公開元URL | https://www.mhlw.go.jp/stf/newpage_27607.html |
| 出典情報 | 薬事・食品衛生審議会 薬事分科会医薬品等安全対策部会安全対策調査会(令和4年度第10回) |
ページ画像
ダウンロードした画像を利用する際は「出典情報」を明記してください。
低解像度画像をダウンロード
プレーンテキスト
資料テキストはコンピュータによる自動処理で生成されており、完全に資料と一致しない場合があります。
テキストをコピーしてご利用いただく際は資料と付け合わせてご確認ください。
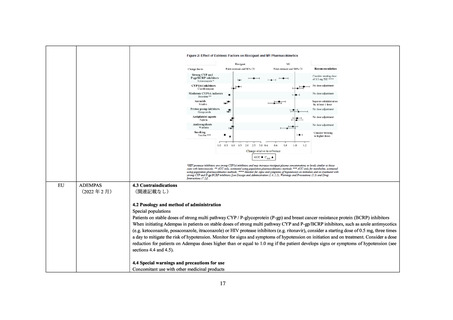
4.4 Special warnings and precautions for use
Concomitant use with other medicinal products
• The concomitant use of riociguat with strong multi pathway CYP and P-gp /BCRP inhibitors such as azole antimycotics (e.g.
ketoconazole, posaconazole, itraconazole) or HIV protease inhibitors (e.g. ritonavir) results in a pronounced increase in riociguat
exposure (see sections 4.5 and 5.2).
• Assess the benefit-risk for each patient individually before prescribing Adempas in patients on stable doses of strong multi pathway
CYP and P-gp/BCRP inhibitors. To mitigate the risk of hypotension, consider dose reduction and monitoring for signs and symptoms
of hypotension (see sections 4.2 and 4.5).
• In patients on stable doses of Adempas, the initiation of strong multi pathway CYP and P-gp/BCRP inhibitors is not recommended as
no dosage recommendation can be given due to limited data. Alternative treatments should be considered.
カナダ
ADEMPAS
(2020 年 3 月)
4.5 Interaction with other medicinal products and other forms of interaction
Concomitant use with strong multi pathway CYP and P-gp/BCRP inhibitors
Highly active antiretroviral therapy (HAART)
In vitro, abacavir, rilpivirine, efavirenz, ritonavir, cobicistat and elvitegravir inhibited CYP1A1 and the metabolism of riociguat in the
order listed with abacavir as the strongest inhibitor. Cobicistat, ritonavir, atazanavir and darunavir are additionally classified as CYP3A
inhibitors. In addition, ritonavir showed inhibition of P-gp.
The impact of HAART (including different combinations of abacavir, atazanavir, cobicistat, darunavir, dolutegravir, efavirenz,
elvitegravir, emtricitabine, lamivudine, rilpivirine, ritonavir, and tenofovir) on riociguat exposure was investigated in a dedicated study
in HIV patients. Concomitant administration of HAART combinations led to an increase in riociguat mean AUC of up to about 160% and
to an approximate 30% increase in mean Cmax. The safety profile observed in HIV patients taking a single dose of 0.5 mg riociguat
together with different combinations of HIV drugs used in HAART was generally comparable to other patient populations.
To mitigate the risk of hypotension when Adempas is initiated in patients on stable doses of strong multi pathway CYP (especially
CYP1A1 and CYP3A4) and Pgp/BCRP inhibitors, e.g. as contained in HAART, consider a reduced starting dose. It is recommended to
monitor these patients for signs and symptoms of hypotension (see sections 4.2 and 4.4).
CONTRAINDICATIONS
(関連記載なし)
WARNINGS AND PRECAUTIONS
Hypotension
As a sGC stimulator, ADEMPAS acts as a vasodilator, lowering both pulmonary and systemic blood pressure. The demonstrated risk of
hypotension should be carefully considered (see ADVERSE REACTIONS), in particular in patients with concomitant or underlying
conditions such as low systemic blood pressure (e.g., systolic blood pressure < 95 mmHg), coronary artery disease (CAD), hypovolemia,
resting hypotension, severe left ventricular outflow obstruction, autonomic dysfunction, as well as in patients on concomitant treatment
with antihypertensives or strong CYP and P-gp/BCRP inhibitors (see WARNINGS and PRECAUTIONS, Concomitant Use with CYP or
19
Concomitant use with other medicinal products
• The concomitant use of riociguat with strong multi pathway CYP and P-gp /BCRP inhibitors such as azole antimycotics (e.g.
ketoconazole, posaconazole, itraconazole) or HIV protease inhibitors (e.g. ritonavir) results in a pronounced increase in riociguat
exposure (see sections 4.5 and 5.2).
• Assess the benefit-risk for each patient individually before prescribing Adempas in patients on stable doses of strong multi pathway
CYP and P-gp/BCRP inhibitors. To mitigate the risk of hypotension, consider dose reduction and monitoring for signs and symptoms
of hypotension (see sections 4.2 and 4.5).
• In patients on stable doses of Adempas, the initiation of strong multi pathway CYP and P-gp/BCRP inhibitors is not recommended as
no dosage recommendation can be given due to limited data. Alternative treatments should be considered.
カナダ
ADEMPAS
(2020 年 3 月)
4.5 Interaction with other medicinal products and other forms of interaction
Concomitant use with strong multi pathway CYP and P-gp/BCRP inhibitors
Highly active antiretroviral therapy (HAART)
In vitro, abacavir, rilpivirine, efavirenz, ritonavir, cobicistat and elvitegravir inhibited CYP1A1 and the metabolism of riociguat in the
order listed with abacavir as the strongest inhibitor. Cobicistat, ritonavir, atazanavir and darunavir are additionally classified as CYP3A
inhibitors. In addition, ritonavir showed inhibition of P-gp.
The impact of HAART (including different combinations of abacavir, atazanavir, cobicistat, darunavir, dolutegravir, efavirenz,
elvitegravir, emtricitabine, lamivudine, rilpivirine, ritonavir, and tenofovir) on riociguat exposure was investigated in a dedicated study
in HIV patients. Concomitant administration of HAART combinations led to an increase in riociguat mean AUC of up to about 160% and
to an approximate 30% increase in mean Cmax. The safety profile observed in HIV patients taking a single dose of 0.5 mg riociguat
together with different combinations of HIV drugs used in HAART was generally comparable to other patient populations.
To mitigate the risk of hypotension when Adempas is initiated in patients on stable doses of strong multi pathway CYP (especially
CYP1A1 and CYP3A4) and Pgp/BCRP inhibitors, e.g. as contained in HAART, consider a reduced starting dose. It is recommended to
monitor these patients for signs and symptoms of hypotension (see sections 4.2 and 4.4).
CONTRAINDICATIONS
(関連記載なし)
WARNINGS AND PRECAUTIONS
Hypotension
As a sGC stimulator, ADEMPAS acts as a vasodilator, lowering both pulmonary and systemic blood pressure. The demonstrated risk of
hypotension should be carefully considered (see ADVERSE REACTIONS), in particular in patients with concomitant or underlying
conditions such as low systemic blood pressure (e.g., systolic blood pressure < 95 mmHg), coronary artery disease (CAD), hypovolemia,
resting hypotension, severe left ventricular outflow obstruction, autonomic dysfunction, as well as in patients on concomitant treatment
with antihypertensives or strong CYP and P-gp/BCRP inhibitors (see WARNINGS and PRECAUTIONS, Concomitant Use with CYP or
19